My Mom’s Heart Attack Went Undetected for 20 Days. Here’s What I Learned.
The Day That Changed Everything
I was traveling abroad when I got the message that no one wants to receive.
For twenty days, my own mother had been suffering. Twenty days of what she described as severe indigestion and cramping, a feeling she said came from her stomach. She went to doctors. They ran tests. They sent her home. They told her it was probably acid reflux, maybe stress. The symptoms persisted and she was referred to visit one specialist after another, until finally on week 2, they recommended an MRI and Xray. It was on the 19th day when her Radiologists identified an abnormally swollen heart.
I flew back and immediately took her to the emergency room myself, they ran an EKG. It came back normal. They ran an ECG. Normal. The machines that we trust to catch heart attacks — the same technology that has been the gold standard for decades — saw nothing wrong.
Twenty days.
What saved my mother’s life was a doctor in the ER who finally said, “Let’s run a blood test.”
That test was called a high-sensitivity troponin assay. It measures cardiac troponin — a protein that only exists in heart muscle cells. When those cells die, they release troponin into the bloodstream. My mother’s blood was full of it (237 to be exact).
She had been having a heart attack for twenty days. Not the dramatic, chest-clutching kind you see in movies. A silent one. An NSTEMI — a Non-ST-Elevation Myocardial Infarction — the type that doesn’t show up on a standard EKG or stethoscope because it doesn’t produce the classic electrical signature doctors are trained to look for.
Her heart had been failing, and no one knew.
This Happens More Often Than You Think
After my mother’s diagnosis, I started researching. What I found was disturbing.
Women are 50% more likely to be misdiagnosed during a heart attack than men. For NSTEMI specifically, women have a 41% greater chance of receiving the wrong initial diagnosis (European Society of Cardiology).
Why? Because medical education has historically centered on male patterns of presentation. The “classic” heart attack— crushing chest pain radiating down the left arm — is a male symptom. Women are more likely to experience:
- Shortness of breath
- Nausea
- Back pain
- Fatigue
- And yes — indigestion and stomach cramping
My mother’s symptoms weren’t unusual. They were typical — for a woman. But the diagnostic tools weren’t designed with her in mind.
In a study from the Global Registry of Acute Coronary Events, approximately 33% of heart attack patients present without chest pain (Canto et al., JAMA 2000, 434,877 patients). For patients over 85, over 40% with NSTEMI have non-diagnostic ECGs. The machines we rely on are missing critical cases.
And when diagnoses are missed, people die. Hospital mortality for NSTEMI patients without chest pain: 15.3% versus 5.4% for those with typical symptoms — a 2.83× increased risk (Canto et al., NRMI registry, 1,143,513 patients). This gap is why atypical presentations are so dangerous.**
The 200-Year-Old Technology Still in Every Hospital
Let me tell you about the stethoscope.
In 1816, a French physician named René Laennec was examining a young woman with symptoms of heart disease. He was uncomfortable placing his ear directly on her chest — the standard practice at the time. So he rolled up some sheets of paper into a tube, placed one end on her chest and the other to his ear.
He was astonished. The sounds were clearer than he had ever heard.
Over the next three years, Laennec perfected his invention, eventually carving a wooden tube that became the first stethoscope. He named it from the Greek words stethos (chest) and skopos (examination).
That was over 200 years ago.
And here’s the problem: hearing is subjective. What one doctor hears as a murmur, another might miss entirely. The interpretation depends on the observer’s training, experience, hearing acuity, and even the ambient noise in the room.
By definition, this introduces variability. In science, variability is the enemy of accuracy. When the same patient can receive different interpretations from different doctors using the same tool, we have a problem.
Modern ECG machines improved upon this — they produce objective electrical tracings. But they introduced their own problems: intimidating electrodes, clinical environments that trigger anxiety, and fundamental limitations in what they can detect.
Let’s face it, who wouldn’t get anxious when the cold metal electrodes are placed on your chest. If you’re at risk for Cardiovascular disease, the last thing we need in a clinical setting is to elicit fear and anxiety.
The Irony of Cardiac Monitoring
I always wondered why we still use these cold electrodes and long wires that look like they came from a 2000s sci-fi movie. It’s intimidating, it makes me nervous, and it makes my heart pounce.
After a little digging, I learned that 20–50% of patients experience elevated readings due to anxiety, not underlying disease. The same spikes in your heart-rate that you may get when you’re in a hospital, “White coat hypertension.”
Studies have found that even the anticipation of having blood pressure measured triggers a physiological stress response.
Now imagine you’re heart has been failing for nearly 20 days.
For patients already experiencing cardiac symptoms, this environment can exacerbate their condition. The very tools designed to diagnose them can make accurate diagnosis harder.
I’m no doctor but after living through this shared experience where the system that failed her, test after test, doctor after doctor, twenty days of a heart attack that no machine could see. I had to understand how the systems worked, what we have today, and what’s in store in the near future.
The Core Requirements
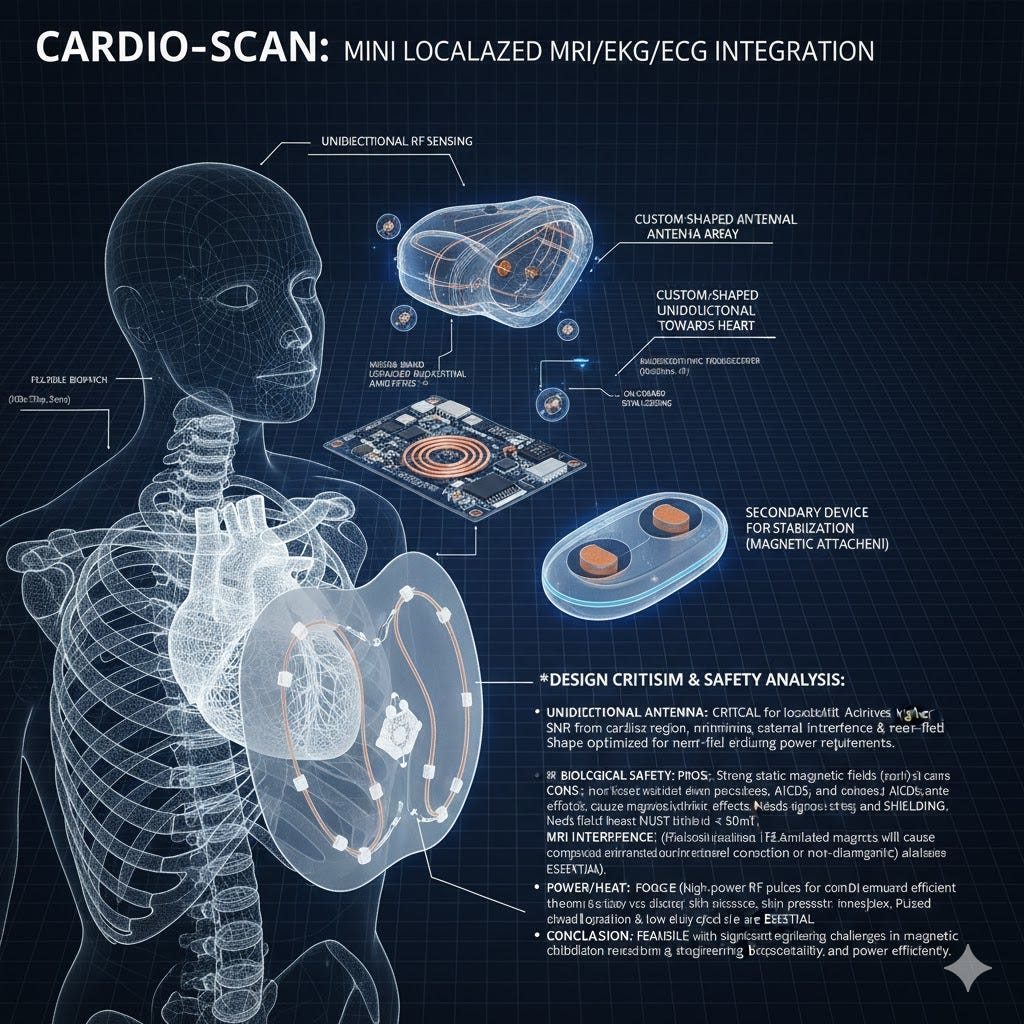
Conformal design: The device curves to match the anatomy of the chest, sitting between the ribs to minimize air gaps and maximize signal quality. Every millimeter closer to the heart increases signal-to-noise ratio exponentially.
Unidirectional field: Using a Halbach array configuration, the magnetic field is focused into the chest toward the heart, not radiating outward. This means lower power, deeper penetration, and safer operation.
Integrated dry electrodes: No cold gel, no intimidating wires. Gold-polymer contact points are built into the device perimeter, capturing ECG signals while the device simply rests on the chest.
Bio-adhesive fixation: Early designs considered magnetic back-plates, but rigorous analysis revealed this could interfere with pacemakers and ICDs. Instead, we use a gentle adhesive polymer — similar to a TENS unit — that holds the device in place without any risk to patients with implants.
The more units of measurement/data inputs, the higher the fidelity, and the more of a logistical nightmare for margains. It doesn’t seem too terrible:
- ECG/EKG functionality — electrical activity monitoring
- Localized NMR imaging — the same magnetic resonance technology as MRI, but miniaturized
- Optical sensing (PPG) — photoplethysmography like Apple Watch heart monitoring, capturing blood oxygen and pulse waveforms
- Acoustic sensing — a high-sensitivity digital microphone that replaces the stethoscope, capturing heart sounds with machine precision instead of human hearing (i.e. MEMS)
The thing is, every component exists today — maybe just not in the form and function we’re hoping for, yet.
V1 Concept Render:
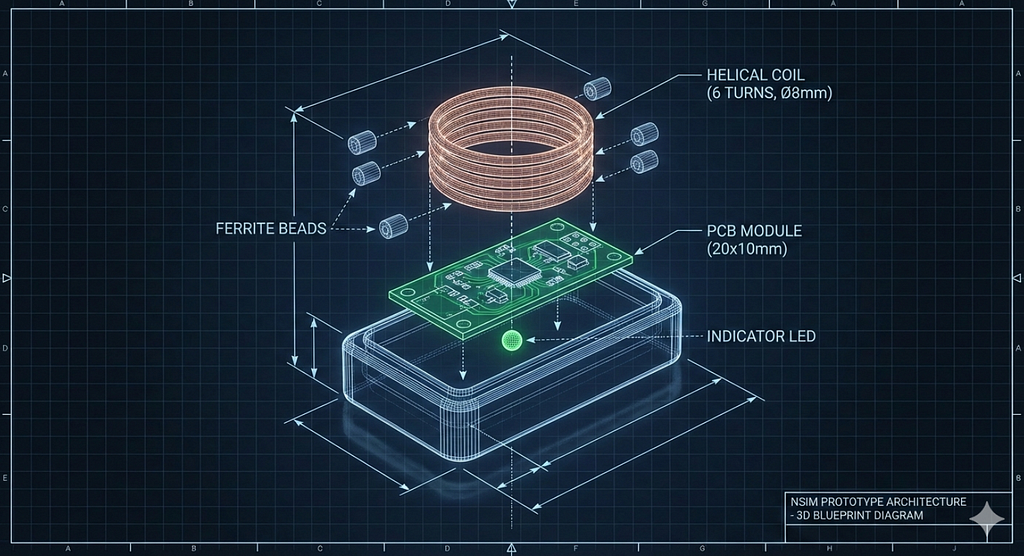
V2 Prototype Mockup:
Conceptualizing a conductive (and warm) backplate for stability… Since MRIs today require really cold temperatures and of course a faraday cage. I challenge you to ask yourself whether fundamental physics constraint, or just a generational limitation.
The Future Is Bright
MRI machines revolutionized diagnostics but they’re expensive and inaccessible. Wearables brought monitoring to our wrists but sacrificed depth for convenience. ECGs have been the cardiac standard for decades but miss the very conditions that kill women at disproportionate rates. Apple is making brain-monitoring airpods.
It’s only a matter of time. I’ve seen a vast number of handheld monitoring patents being filed, I hope this blog inspires one of the inventors, and the inventor in you.
It’s only a matter of time.
“One of the great challenges in life is knowing enough about a subject to think you’re right, but not enough about the subject to know you’re wrong”
Written with AI assistance (Claude). All claims verified by the author.